This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
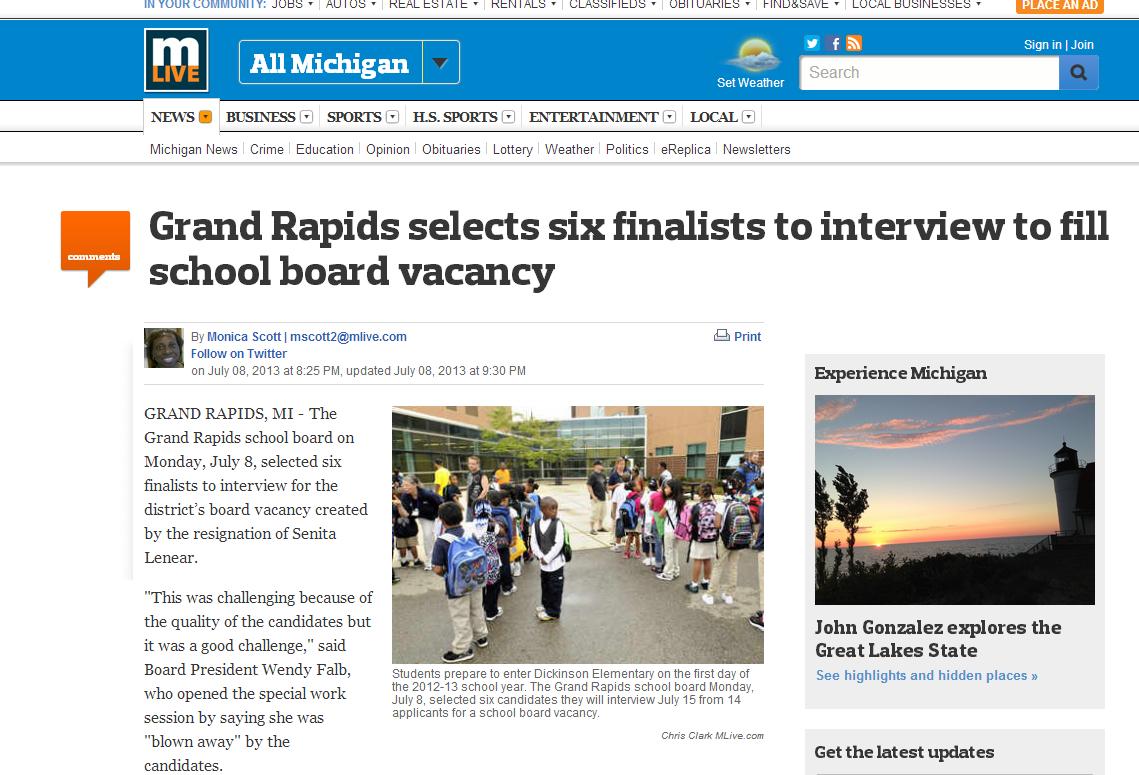
Monday, I had the amazing opportunity to be interviewed for the Grand Rapids Board of Education. I was one of six finalists selected for the public interviews. Ultimately, I was not chosen, but I was very thankful for the opportunity, and I left the interviews with an amazing sense of enthusiasm about how our community is banding together around students. I wanted to share a few thoughts with you that I distilled from my interview comments.
Education and Innovation
I think the single biggest thing I offer the world, ultimately, is that I have substantial experience in being an innovator inside the “big box.” That is, I know how to think like an entrepreneur, read the market or environment, and act quickly and decisively, while interfacing with the complexities of a large, established organization. I’ve done this a number of times in my past, as an engineer, and I am doing this today innovating for kids with autism at Hope Network. In particular, my work there emphasizes mission-driven entrepreneurship in the non-profit sector. I think education could use more of this kind of thinking. Most public school systems are likewise large, mission-driven organizations in need of innovation. If they team up with people who know how to innovate within the “big box,” as they create game changing educational solutions, innovators can help them engage and captivate the public attention so that they get the community support they need to succeed.
Education and Collaboration
In truth, I’ve really never had a job where I didn’t have to collaborate on a team. I mean, in high school, when I bagged groceries at Family Fare, I was on a team with the other baggers and cashiers – we looked out for each other, flexed to help each other so no one had to shoulder too much work, and so on! I’m not sure I know what it means to go solo, or that it makes any sense in the modern world. I approach teams at three levels. On one level, I may be a subject matter expert on the team, and I advocate for evidence-based or evidence-informed practices based on my expertise. On another level, I learn from every team, and whenever I’ve participated on a team, I’ve surreptitiously become a minor expert in some topic on which I would never have spent time had I not been on that team. Finally, I think all team members should try and play a facilitative role for each other, to make sure views are heard, that expertise is shared, and that the team together is able to make informed decisions. That’s when a team becomes stronger, rather than weaker, than the sum of its parts. I think all of these things are important in many ways in the school setting. Collaboration between administrators and teachers. Collaboration amongst teachers. Collaboration among teachers, students, and families. And finally, community collaboration so that education extends far beyond the school walls.
Education and Diversity
I think the biggest thing I try to do to promote diversity is to push everyone to understand how they bring diversity to the table and to think constructively about their own viewpoints, how they align or differ with those of others, and how they can be strengths or barriers. I listen to people, and I help them bring out their own unique view. I respect those views, even when they run contrary to mine, and I help them be the best “them,” rather than trying to make them into someone they are not. Personally, I feel this is a much better approach than trying to address diversity by demographic matching or telling some people they are “diverse” and other people they are “not diverse.” Some of this comes from the fact that Indian Americans are a relatively small group within the population. If Indian Americans were on this board in proportion to how many live in the city, I might never be “represented.” In my early career, I was provided mentors on several examples and I was always placed with a senior Indian or Indian American in the organization, without any attempt to understand me, my fit with that person, or how that relationship would contribute to my development. I don’t think that’s diversity. That’s pretend diversity. But if we encourage diversity in the broader sense, then we can have a real diversity and build a sustainably inclusive community. This is a process that can start very early – when I interviewed yesterday, I heard a really touching story from one of the other candidates about how she learned to be inclusive as a special needs preschooler (she’s now a very successful consultant). I didn’t learn inclusivity until much later. Think of what we could do and be if all our kids learned to be inclusive at three or four years of age.
Education and Liberty
In interviewing for my school board, I did some thinking about why we care about institutions like public education. I believe passionately that what makes our society a great one is that we have invested for more than two hundred years in “technologies” and innovations that enhance freedom and liberty. We have never been happy to say we are “free enough” and hang our hats, and even as we talk today, we are engaged on many fronts as Americans in trying to make ours a freer state and nation. Public education is a great innovation because it makes people freer. There is hardly anything in the world that does more to free people than the work schools do. And thus, there is hardly anything more American than to stand beside schools, take up arms with them, and make the next generation and the next one after that freer and freer through the gift of knowledge through public education.
These are just a few reflections I had on education, many of which I connect back to my approach to being an autrepreneur. I hope perhaps I fueled some thought processes of your own about how to bring education and innovation together. I don’t mean to pretend to know more than teachers, but I do feel that we entrepreneurs and autrepreneurs may have some things we can bring to the table. What do you think?
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
Editor’s Note: Welcome back, Neha! If you missed it, here is her excellent first guest post here, sharing her unique perspective as an autism sibling.
No matter how much I try to explain what autism is and how it affects my life, it can never be enough. Writing about it and explaining in personal can only teach others so much. Only through actually seeing how it manifests with your own eyes will you understand what autism really is. Only by visiting an autism household randomly (we’re skilled at last minute clean ups and faking smiles) will you see how the constant mess, craziness, and stress takes a toll on every single member. Some days, you can literally feel stress in the ait. It chokes you and strangles you, as if the very air around you is trying to close your throat, but you have to continue gasping for air. You have to keep gasping until the night is finally complete with the hope that the next day will bring a fresh start. At times, you have to continue gasping and fighting for days on end. Worry not, eventually you shall be able to breathe freely again. The muscles around your neck have strengthened, your body is stronger and is able to free you from the hands of tension that once attempted to choke you. Your determination shines through the haze of depression that surrounds you. Others may not see the warrior within you that faces the constant battles until they understand what autism is. Then, they will see how truly amazing each member of an autism family is.
I wrote the paragraph above on a day where that wasn’t as stressful as the days that followed. But no matter how much I try to explain this view of autism, no one will fully understand until they’ve seen it and been through it. I wish other people could see how hard working some of these autism parents are, how they battle every day, how siblings are the shaky understudies of these heros. I realise this post may be a bit depressing to read, but it’s honest. Sometimes, you have to confront the bad and cancel it out with good (or greatness or brilliance, you choose). We have to start somewhere if we want a better future for autism families!
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
First of all, I’m sorry for not writing more content for my blog recently. We’ve got something very exciting coming up at my Center, which is still unfortunately under wraps. It’s going to be public knowledge soon, but let me just say it’s incredibly exciting, and it’s kept me incredibly busy.
I’ve also been a little reticent to post on the topic of the DSM-V, for a variety of reasons, although I’ve tweeted about it and e-mailed privately with people I value highly in the autism community. This is in part because my own view, as a pragmatist, has been evolving, and in part because, the more I think about it, the question of whether the “DSM-V got it right” is really fundamentally the wrong question to ask.
Dr. Thomas Insel of NIMH wrote a post a few months ago that many of you have read. I think it raises some great points while simultaneously being somewhat disingenuous. He raises an analogy between how we diagnose complex neurodevelopmental disorders like autism and how we diagnose heart attack. I think this is as unreasonable as comparing how we diagnose cancer with how we diagnose leg fractures. Let alone that heart attack is ultimately an acute illness and autism is a developmental concern, this creates a false dichotomy in which psychiatric diseases are arbitrary and non-psychiatric medicine is black and white. I don’t mean this as disrespect to Dr. Insel — rather, I think that he (and the proponents of RDoC) are thinking radically, but they’re actually not thinking quite radically enough. I think this is true in part because RDoC is a NIMH project — a mental health project. Thus, it fails to be radical enough by failing to stop and critically ask how diagnosis occurs in complex disease states outside of of psychiatry. Even just a step as far as neurology is highly informative.
I think epilepsy is a great study, and it’s accessible to me, since I wrote my dissertation on epilepsy, and because, as a neuropsychologist, I’ve spent a large amount of time by the sides of children and adults both who have “neurological” disorders and those who have “psychiatric” disorders. Just briefly about epilepsy, it is a complex cluster of disorders that have the common feature of recurrent, unprovoked episodes of electrical abnormality in the brain (that is, epilepsy is, in essence, seizures that occur recurrently and at least sometimes in the absence of an acute medical cause such as fever). Diagnosing epilepsy is complicated — although there are some very well understood forms of epilepsy, in many complex cases, multiple diagnostics (EEG, MRI, PET/fMRI, MEG neuropsychological evaluation, etc.) can provide only partially overlapping results. Thus, some cases of epilepsy are not purely algorithmic — there is no conceptual machine whose crank can be turned and spit out a reliable diagnosis without use of clinical skill, at least not in all cases. Many cases of epilepsy are also “idiopathic,” or “cryptogenic,” meaning that, although we have possible models for how they came to be and why they occur, we don’t really understand their biological basis. The diagnosis of epilepsy is also evolving over time as new instruments and techniques come into use. Thus, epilepsy highlights the fact that complex disorders are not black and white, even outside of psychiatry. The ICD-9 has diagnostic groupings for epilepsy. The ICD-10 has diagnostic groupings for epilepsy. Note how very common conceptual classifications of epilepsy, like medial temporal lobe epilepsy, with mesial temporal sclerosis, are not in either the ICD-9 or -10. And yet the world does not end, and unlike children with autism, children with epilepsy (including children with autism and epilepsy) actually get access to proper and efficacious treatments … for their seizures. How do they do this? By way of classification schema that focus solely on the question of how we do best by people with seizures, rather than on some broader and amorphous question like “what is mental illness?”
This is where disingenuous comes in. These other complex disorders have in common that, although there are ICD diagnostic classifications (which change only slowly), there is international consensus driven by experts in that field who are mutually accountable and accountable to stakeholders in that same disorder community. It is the International League Against Epilepsy, ultimately, and not the American Academy of Neurology, that has traditionally taken the lead on epilepsy classification, and they do so with an eye to making progress in epilepsy, not worrying about whether there is some grand scheme in which the needs of people with seizures are not over-weighted against the needs of people with peripheral neuropathy. In contrast, in the DSM process, members of the autism professional community are picked by a team of psychiatrists, and then paraded in front of psychiatric review committees, and autism is put in the position of selling a diagnostic criteria onto psychiatry, for absurd reasons such as limiting the overall rate of psychiatric diagnosis. A sensible diagnostic process has to be driven by autism stakeholders, and not as part of some package deal for psychiatry, and this is not going to happen if “mental health” is held in a ghetto for “disorders” that aren’t “real.” (Which is a concept no parent of a non-verbal child with autism has ever worried about!).
The second major distinction between other complex disorders, epilepsy again as an example, and the way autism is treated today, is that it is well accepted outside of psychiatry that, in the post-modern era, knowledge can advance rapidly, and definitions will not be static. The diagnostic basis for autism should change when the data says it should change, not when there is a decision to make a new DSM. Other fields get by fine with making as-needed changes to the accepted practice for a disorder, without changing the related ICD codes. Note that this discussion does not really occur in other complex aspects of medicine — in spite of how quickly, for instance, cancer knowledge has been changing (while we are implementing, in the USA, an ICD that is already 20 years old). As far as I know, other fields dealing with complex disorders do not have or need a “bible” governing practice, but rather have many practice guidelines that are updated as needed and specific to diagnostic groups and entities.
So, my point in examining epilepsy is that, really, asking if the DSM-V got it right is the wrong question, because the DSM itself has become the answer to the wrong question. RDoC is a nice idea, but I’m not sold on it, particularly because it continues the tradition of an arbitrary ghetto that pulls psychiatric disease together and apart from other kinds of diseases (thus, for instance, emphasizing similarities and differences between autism and schizophrenia, over similarities and differences between autism and epilepsy). And, it is really not necessary, even with very complex disorders, to have a central “bible” that sets criteria in stone, in order to make progress (rather, to the point, one would have to ask why psychiatry has not far outstripped all other medicine, having had this advantage for decades).
In this way, I worry that the NIMH itself is as flawed a way to solve this problem as the APA (their APA, not ours) is. The real solution should start with the radical concept of simply considering these psychiatric disorders in the same way we consider complex disorders in other parts of medicine. I honestly do not know exactly what the answer is. I think there are almost certainly differentiable neuroendophenotypes within autism, and I think that mixtures of neuropsychological results, genetics, neurodiagnostics, and other markers will likely enable us to diagnose them correctly. I personally doubt that they happen to take the form of the DSM-IV framework. But, I think, in order to solve this riddle, we need to focus on autism and not engage in grand bargains, whether they be NIMH or APA driven.
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
Editors note: please give a warm AutismFamily welcome to Neha Siddiqui, our first guest poster!
This is my first post here, hello everyone! I’d like to start by asking you all to watch the video I have linked, in this video I am speaking to over 100 people about autism from my point of view. Below is the transcript of the video, followed by a hint of what my next post will be about. Enjoy!
“What is Autism? The official definition is, “a group of complex disorders of brain development, characterized by difficulties in social interaction, communication, and repetitive behavior.” It affects each person to a different degree, which is why it’s classified as autism spectrum disorder. Now, how many people actually understood what I just said? Basically, their brains are just wired differently. To me autism is so much more than just a textbook definition, it really affects every single aspect of your day-to-day life, whether you’re the one with autism or you live with someone who has autism. Something of this magnitude can’t be fully explained or even understood in a few minutes, but I’ll try my best to share my experiences and knowledge with you today.
I have an 18-year-old brother – an amazing brother who has autism. 13 years ago my family and I used to live in Ireland, and when I was 7 years old my brother was diagnosed with Autism. Due to the lack of resources available for autism in Ireland in 1999, we decided moved to Australia. But there, we found that the school he was to start attending was for only kids with Autism, and my mother wanted him to be in a more mixed environment, more mainstreamed. Only after a month, we made the move to Houston, Texas y’all and we’ve been there ever since. It’s safe to say Autism has impacted my life in a big way, but think of what it’s like for my brother. Think of what life is like from his perspective.
My brother has moderate to severe autism, and because he’s semi-verbal, he cant pronounce words like we do everyday. His muscles just don’t work that way. This is what I meant by communication difficulties people with autism face everyday. So, when he’s in school, how is he supposed to tell anyone he’s thirsty or needs to use the bathroom? If he’s angry or sad how is he supposed to express himself? In fact how am I supposed to figure out what he’s upset about, so I can solve the problem? Well, thankfully there are ways to overcome verbal communication. My brother, Sameer, was taught a bit of sign language in school. When he’s thirsty, he can sign for water or sign to eat when he’s hungry. I’m so used to routinely asking Sameer, “Yes or no,” in sign language that I automatically start to sign in daily conversation. Some kids who can’t speak at all learn how to type and are able to communicate very intelligently. Take Carly Fleischmann for example, a girl from Canada who has severe autism and apraxia, which prevents her from speaking. She’s able to type and now even has her own blog; this is a girl who was never able to talk to her parents, she couldn’t say she wanted to eat this and not that, or that she didn’t want to wear a sweater today but just a cardigan instead. At age 11 she learned how to type and let the world know how she really feels and why she acts the way she does. There are numerous other kids who have been able to overcome their lack of communication and write beautiful poems of life from their eyes, and how they feel trapped in their own bodies.
Sensory Processing Disorder is another condition most people with autism have. It’s when sensory signals in the brain don’t get organized into the appropriate responses. Think about your 5 senses and how much you rely on them to provide you with information from your surrounding environment; you can see what’s going on, hear other people’s voices, etc. For people with autism, these five senses are all magnified. Sameer has never worn jeans in his life, not because he’s picky, but because the material is too rough and hurts his skin. Another example is that Sameer wears his sunglasses year round, day and night, because he’s really sensitive to light. He even falls asleep in them sometimes! He’s even more sensitive to sound, though. If I’m asking him a question, the buzz of a cell phone on vibrate may be as loud as my voice. He can’t filter out the extra noise around him, whether it be the hum of electronics or someone’s voice down the hall and in another room. If I keep repeating my question and raising my voice because he didn’t answer the first time, it’s just going to frustrate us both and cause pain to Sameer’s ears. Because Sameer can’t communicate to me verbally and say, “Can you please lower your voice, I’m trying to filter out the noise around me,” he may communicate this through his behaviour. He may scratch me or dig his nails into my arms, but this isn’t a behaviour problem. This stems from an inability to communicate.
If this happened in public, and this is a mild example of him digging his nails into my arm, people start to stare and move away. This is nothing compared to the stares received when my brother displays repetitive behavior or does self-stimulating activities. Everyone does self-stimulating activities, like tapping your pen on the desk, biting your nails, pacing back and forth, but for people with autism it’s to help them handle sensory overload. There’s too much going on, too much noise or light; Carly, the girl who communicates through typing, said, “It’s way for us to drown out all sensory input, that overloads us all at once. We create output to block input.” This may be through humming, flapping hands, by playing with a string, or a number of other ways. Now, if there is a 6 ft. tall boy wearing sunglasses jumping up and down and flapping his hands, people tend to stare. Not just stare and walk away, but stop and stare. When I was younger, I would be embarrassed to go out in public with my brother because of how much people would stare and single us out. But now that I’m more confident, I can go with him anywhere.
OCD and anxiety issues are also very common with kids who have autism, which makes going anywhere a problem, sometimes even from room to room in a house. They have a set routine they have to fulfill before doing anything, Steps 1, 2, and 3 have to be done in that perfect order, at the perfect time, or you are not moving on. Let’s say there’s a kid who has to run a lap in his backyard every morning before he goes to school. This kid will run outside even if it’s raining, snowing, there’s a tornado, or a hurricane, this child will run his lap or else he’s not going to school.
These are just some things parents and siblings deal with on a daily basis. And because these experiences are so different from what other families face, it’s difficult to talk to anyone else about this; in a sense, it isolates us. This is one of the first times I’m opening up about this, I couldn’t talk to any of my friends in high school about how my brother has a childhood habit of playing the same scene from VHS tapes over and over again, or how we have stacks of VHS tapes that are 6 ft. tall. I couldn’t explain how frustrating it is when Sameer listens to the same part of “You Found Me” by The Fray for days, it can make you go crazy and really test your patience. Not many understand the implications of this. When I get angry or irritated, my mother always makes me think of his point of view, that this is his form of entertainment and I have my entertainment. I need to understand this, be more patient, and move on. I mean 4 years later, I don’t even hear the song when it’s being played. You really have to take it one day at a time in our house. As you can see, we don’t have a typical brother-sister relationship; I can’t sit and have a conversation with him about what he thought of a movie or as his opinion. Despite that, we have a strong relationship and our bond is deeper than most siblings. This may be because we’ve been through the toughest of times together, and you have to hit the lows in order to reach the highs. Because it is such a high stress life at times, you do see mental health problems, such as depression and anxiety, in family members. As I said, our experiences differ from everyone else, so we tend to isolate ourselves and not talk about it, which increases the chances of mental health problems occurring.
A new study in US weekly suggests that kids with autism have an increasing risk of suicide and depression, and bullying is one of the main factors for this. These kids are more susceptible to bullying because they are different and easy to take advantage of. Currently there’s a campaign by an Olympic torch bearer and Autism Ambassador, Kevin Healey, to try and change laws against bullying and harassment of people, especially adults, with autism. This includes an online petition, connecting with celebrities all around the world, to try and raise awareness of this issue. As he tweets about the campaign, he receives death, which shows you the seriousness of the issue. This campaign reminds me of why I want to be a doctor in the first place- so I can help improve the situation of other families like mine, to decrease their suffering so they won’t have to struggle like we do. I wouldn’t be half the person I am today if it my brother wasn’t the way he is. I wouldn’t be able to understand other peoples difficulties or be so empathetic if my brother wasn’t the way he is, and I definitely wouldn’t be so motivated in what I do every single day. I have an amazing 18 yr old brother who has autism and I’m blessed with a big responsibility to take care of him and be an advocate for those with autism. I wouldn’t trade it for the world.
There are many aspects to autism that I probably missed, but I hope I’ve done enough to decrease some of the stigma surrounding autism and all of you leave with a better understanding of what life is like from another perspective. Thank you.”
If you’re a sibling of someone who has autism, know that you are brilliant. Whether you realise it or not, you’re amazing. I’m not just saying that to make you feel better about yourself, I’m saying this because I know it. It’s taken me twenty years to be able to put my life experiences into words, and it was only after I went to college that I learned how different life is for everyone else. To me, life is so boring without my brother. My next post will be about how much I’ve learned to appreciate every day with my brother, and how you can appreciate your siblings too!
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
This is a lecture I gave at our FamilyRounds educational program last week. The embedded video is the actual lecture, and an edited transcript follows below. Enjoy! And … if you’re a member of the AutismFamily, please pass this along and take a few moments to think about how you can commit yourself to being well, for your own sake, and for the sake of your family members.
My usual lectures involve a lot of details, a thorough review of the latest scientific literature, with examples from my clinic and both existing and possible future applications. I rely heavily on data, numbers, which makes sense if you understand my specialty. But when I started thinking about this topic of emotional wellbeing for the AutismFamily, however, I came to the realization that this is not a story that needs to be told with a lot of new data, or a synopsis of findings from the latest scientific literature. This is a different story, which begans with truths all of you – all of us – know, but struggle to employ in our daily lives.
I hope this post and lecture can be the beginning of an honest conversation about how we bring this concept to the AutismFamily and learn – together – how to be and stay truly well. If we do this right, wellbeing is both an aspirational goal (one we progress towards our entire lives, going ever farther) and a daily reality. But let me start with what wellbeing is, and why it matters. The World Health Organization defines health as “a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity.” That is, it is not our jobs to merely not be sick, but to thrive. It is not enough to merely not die, but we must also live. The WHO, which is mostly concerned with so-called “physical” diseases (acquired injuries, consequences of malnutrition, heart disease, and so on), astutely included not just “physical” wellbeing but also emotional wellbeing in their definition. The truth is that there really is no difference between the two. The brain and body are interconnected – that’s the whole point of having a brain. Research has shown that measurable “brain” factors like a disposition towards positivity can actually have effects on cancer outcomes that in some cases, may even be comparable in magnitude to choice of chemotherapy agent (here’s another example for cardiovascular disease). Studies have shown that depression is a much bigger risk factor for a heart attack than smoking (here’s another cardiovascular summary). And when people do suffer from both “physical” and “psychiatric” disease, the cumulative effects are frequently far harder for them to manage. Most of the disability associated with chronic medical illness is explained by whether or not the person is also depressed, not the severity of the illness. Across many illnesses, depressed people are three times less likely to be able to successfully remain adherent to their medications (my dissertation has an extensive review of this literature). Hopefully these statistics provide an introduction to why and how the way we feel emotionally is every bit as important as the way we feel physically, if not more so.
There’s one more reason that all of this is particularly important for the AutismFamily. As parents, you need to take care of yourselves, so that you can take care of your children. You’ve all heard this one, boarding a plane: “In case of a sudden loss of cabin pressure, inflatable air masks will drop …” They tell you, if you are traveling with a child, secure your own mask before you help your child get their mask on. It counters every impulse most parents have. Autism parents, especially, drive, fly, run, leap, fight for their children. Every day. How could you even think about taking care of yourself before your child? On the airplane, if you try to put your child’s mask on first, you may pass out in the process due to lack of breathable air. What good would you be, to your child, in an unstable plane at 30,000 feet, unconscious? Where are the places in your life where, if you do not take care of yourself, you cannot be the parent you must be? The moral of the story is that, even if you don’t believe maintaining your own strength is important for you, it’s important for your son. It’s important for your daughter. And with autism, as you all know, this is a cross-continental flight, not a puddle jump. We’re in it for the long haul.
So, taking care of ourselves is important. Again, though, you may know more of these details or less of them, but you know this. The problem is not conceptually or abstractly believing we must take care of ourselves. It is actually doing so. When I describe our intensive behavioral clinic, I talk about what our therapists do as easy to say and hard to do. Like being told that one loses weight by exercising more and eating less. Everyone knows that already. Just knowing that isn’t enough.
So, one of the struggles with where to go from here is the approach we take towards wellbeing, and making it actually work. I am a firm believer in tools like mindfulness and other formal tools that help us feel and be better. There is really solid evidence that mindfulness can assist with helping people recover from significant emotional disturbances, and it can also help them develop a stronger sense of emotional resilience – the ability to bounce back from challenges. The problem with these tools, often, is that they’re not taught in a way that is broadly applicable to our daily lives. If you’ve ever gone to a lecture about meditation or mindfulness, you’ve probably seen a picture a picture of some beautiful person in designer yoga clothes, serene, meditating or doing a yoga pose on the beach at sunset. I think there’s a problem with this mentality. The problem is that most of us do not struggle to feel mindful or spiritually awakened when we meditate on the beach at sunset. We don’t need that kind of help – I think you’d have to have pretty serious problems to be unable to meditate in this kind of situation, don’t you? If we build up emotional wellbeing practices that only work at the beach at sunset, that only work every few years when the family takes an expensive, major vacation, is that really enough? I think what we actually need is this: wellbeing practices that work in the chaos of everyday life, like those described in Jon Kabat-Zinn’s excellent Full Catastrophe Living.
I’d like to spend a few minutes talking to you about mindfulness. The first thing I want to stress is that all of you have experienced mindfulness. People who exercise know it as the zone. Musicians know it as the groove. At some point, doing something (maybe it is yoga on the beach at sunset), you’ve been there. There have been terms throughout the ages to describe this concept – people called it synchronicity or feeling God’s pleasure. What mindfulness is truly about is taking that sensation or state, and making it something you can experience anywhere, anytime, and purely because you want to and not because of the activity involved. So, mindfulness isn’t really an exercise anyone can teach you, but rather, the more exercises you learn that generate a mindful state, the more you know it when you feel it and you can learn your own ways of being mindful when you need to or want to.
One important concept that can be helpful for mindfulness is the “observing I.” There are many different “I”’s – for all of you in the room, you’re probably a husband or wife, a son or daughter, a father or mother, you have a profession, perhaps you have an ethnic identity, maybe you identify with the kind of music you like or clothes you wear. You fluidly access these different identities as they are relevant to the task at hand, so that, you may not approach work as a mother, and you approach your child differently than your parent. So, amongst all of these I’s, the observing I is a special I that emphasizes equipoise. Equipoise means a state of balance. Think about a big cat, like this one. If you’ve ever watched cats stalk their prey, perhaps on the nature channel, you might notice that, when they’re lurking in the grass, they pass through a moment where they are perfectly still. In that moment, they are dedicated to neither attacking nor walking away. When the moment passes, they frequently do either of these two things, but during the moment, they are neither active nor passive, neither engaged nor disengaged, neither approaching nor avoiding. This is the observing I, and it is paradoxically the lack of engagement or disengagement of this I that allows use of the observing I to make us more able to bravely and fully act on our decisions. To take a step back from our decisions (not to avoid acting, per se, but to be disinterested in whether we act or do not) allows us to be mindful in our decisions, and as we do that, we find that we make good decisions and we enjoy them. Once we have this feeling, we become more like this pond, in the middle of a forest, with a tree standing next to it. On a warm summer day, the pond’s surface is a still mirror, a beautiful reflection of nature’s glory. From time to time, a leaf falls from the tree, and when it does, in an instant, it shatters the pond’s beauty. But as the pond, we know that we have survived for ages and will survive for ages more. We know that leaves come and leaves go, and when the leave falls underneath the surface, we the pond will return to our mirrorlike serenity. In this way, mindfulness allows us to do the things that seem impossible. We cannot eliminate fear, but by embracing the presence of fear without engaging in it, we become transparent to fear, and it cannot control us. We cannot eliminate pain, but by embracing the presence of pain without engaging it, again, the pain passes through us, and we do not suffer.
One of the great powers of mindfulness is that, by engaging this observing I, we stop being the victims of our own thoughts. Stop and think about your thoughts. If we are honest with ourselves, our thoughts are not always our friends. Sometimes, when there is a challenge coming up, we “blow it off.” We assume we’re invincible and unstoppable and we don’t study for our exam or save money for when we have to file our taxes, even though we know we’ll “owe.” Too little stress or anxiety is bad, because when we don’t experience any stress, we don’t work hard and we don’t deliver to the level of our talents. But isn’t there such a thing as too much stress, also? For that same exam, we could spend all our time worrying about how hard it is going to be and how we’re never going to pass. So much time worrying that our worries become a self-fulfilling prophecy, when we don’t pass, because all we did was worry instead of studying. So too much stress is a problem, too. Psychology has a name for this concept, the Yerkes Dodson law. Of course, the problem with this information is that telling yourself not to be stressed is like trying to think about nothing. It tends to have the exact opposite of the intended effect.
Back to our thoughts. I said “victims.” Sometimes, I mean it. The same story about stress applies to our thoughts. You’ve heard people say that “good is the enemy of better.” Can’t you think of some examples of this, where you’ve lived with some problem or nag that you should’ve fixed years ago, but since you learned to get by, you just can’t seem to get up and do anything about it? We’ve all done that. We’re probably all doing that. Sometimes, “better is the enemy of good,” too, though. The name for that is perfectionism. I used to think that perfectionism was an asset, and perhaps some small amount of it is. However, perfectionism is probably a good thing far less often than we give it credit for. So we all have thoughts that make us feel bad about ourselves instead of doing good, and we have thoughts that make us feel good about ourselves, and they prevent us from doing even more good. The reality is that your thoughts are often frenemies — they look like friends and, as soon as we drop our guard, wham, they end up doing us wrong. That’s how we become victims of our thoughts. Where mindfulness comes in is that we don’t try to stop having these thoughts (they’re pretty natural, it probably wouldn’t work), and instead we allow them to come and go as they please, but they are always thoughts we have, and never thoughts that have us. We are observant of them but dispassionate towards them. That takes practice – we all think terrible things about ourselves, like, “I’m a failure and I’m always going to be a failure.” Most of the time, we can distract ourselves or knock ourselves on the side of the head, but when we’re feeling really down, it’s hard to be dispassionate towards a thought like that. But, practicing the observer I lets us get there.
I teach mindfulness exercises (and there’s one in the video above), but mindfulness is not an exercise. It is that thing that one learns experientially from doing all these exercises, and the intent is not so much to change you into something that you are not but to remember who you already were – what you felt like when you were in the zone, the groove, you had the flow or the beat or you saw the vivid colors or ran like the wind. In this way, I think mindfulness is a perfect fit to the topic of developing and maintaining emotional wellbeing for the AutismFamily, because the truth is that I don’t want to change you – my service is merely to help you be the best you. Mindfulness then is a tool to embrace all the reasons you cannot care for yourself, and all the thoughts telling you you’d be selfish to care for yourself, rob them of their power, and allow you to do what you must in caring for yourself.
Another exercise that may be helpful is to take a sheet of paper and brainstorm on the things that are the zone, the groove, the mindful times for you. Not the times when you had fun, necessarily, but the times when you felt that, right where you were, when you were, you were doing what you ought to be. Those times when the world felt right. Then next to them, write down when the last time you did those things was. Was it very recently? Was it a year ago? Two? Not since 1976? If you are doing these things that make you feel the zone routinely, that’s a good start. Next, ask yourself how you can be mindful even more often. If you are doing them rarely, you may need to spend some time just having experiences, getting back into touch with what might be the groove for you. Mindfulness practices can help with this, because as you experiment with different activities, they will help you know when you are where you should be.
Yet another, different way to approach this is to suppose someone were giving a speech celebrating your life, looking back from the future, or making a movie about you. How would you want to be remembered? Would you be able to pick 5-10 adjectives that describe who you’d want to be remembered as? You probably have a lot of future ahead of you, but then, if you go back, can you think of times that could be scenes in your movie or the speech, that would tell the story of why those adjectives fit you? These adjectives are your values, and these scenes are times when you were living your values. If you think back on them, you’ll probably be surprised to note that you did not pick all positive or happy scenes, and in fact, many of your values were most lived out in some of your darkest times. That living by your values, doing what must be done, in the midst of the storm, is again what it means to be mindful. It’s what one means when one says that the human spirit triumphs in adversity.
What all this has to do with emotional wellbeing is that one of the most central ways to build and keep emotional wellbeing is to try and live your life in such a way that you are cultivating experiences where you are mindful, not merely experiences that you think will make you happy. This is when you are in the zone, in the groove, when you feel the cat’s sense of equipoise. If you aren’t regularly doing those things that remind you of who you are and who you want to be, the doctor’s orders are that you need this, surely as you need oxygen or food or water. If you are doing these things, but they are rare or special (like when you went hang-gliding or toured the Great Wall of China), then you must think about what you can do on a daily basis that captures this same feeling. If you are doing small things daily, the thing to do is to ask how you can feel this way not just as part of an activity (whether a coffee break or yoga) but how you can bring this way of being into your daily life.
Lastly, as part of this, I want to make a call for togetherness in the AutismFamily. We come from different experiences, different places, and different needs. We bring different strengths and talents. But as a Family, public accountability makes a big difference. As a leader, I must be careful to care for myself, not just because I have to be there for my team, but because I am a model to them. The same is true for you in leading your families. People — my staff, your children — are watching you. So, my parting thought is that, as an AutismFamily, we need to hold each other up. To celebrate each other, but also hold each other accountable and make sure that each of us learns to take care of ourselves, so we can be there for our families, and for each other. Only then will we maintain the strength and energy to build the world we know we must build.
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
I get accused sometimes of being an ABA (Applied Behavior Analysis) proselyte. Most typically by people who don’t know me or my professional field. As a neuropsychologist, I’m really clinically involved in autism on the “front end” — I diagnose kids and develop treatment plans. Because I run my autism program, I get to also use that as a means to drive therapy and hold it accountable. I don’t just evaluate kids and recommend therapies and never see them again, but rather I re-evaluate them, typically annually, to determine if they are growing and gaining skills, to determine if new approaches are merited by new problems or challenges at a new level of development, and to give the family a central collaborator in myself to help their child thrive.
My simple four-step model of treating autism
When I do that, I integrate a variety of approaches — for young children with autism, I almost always recommend a behavioral intervention, whether ABA, PRT (often if ABA cannot be accessed), or family therapy (typically when skill level of the child is higher). Our early intensive behavioral intervention (EIBI) program is the go-to route for children who are below age level in social/functional communication skills, self-care skills, play skills, or other developmental skills in the context of autism, but I don’t just “throw” children into it without thinking carefully. In our approach, I don’t recommend speech & language pathology, family psychotherapy to aid in friendship development, or other in-clinic services until children are at a threshold level of skill (typically I will talk about these therapies once children are around the verbal level of the mean normally developing five-year-old, based on the logic that many group activities for children, including formal schooling, are designed for children starting at about this level). I will also consider medical diagnostics a family and their physician should consider (MRI, EEG, genetic testing/consultation), dietary or other complementary interventions, academic recommendations, and informal things the family can do at home. I rarely recommend medication before age five years, but after that I will recommend medications where appropriate, largely following the kind of guidelines in this practice parameter. In this context, ABA-based interventions like the EIBI package are my go-to behavioral intervention because they’re the most effective. I’m not a behavior analyst, although I am an affiliate ABAI member. Let me be clear that I choose ABA for my kids because it has the evidence, and because the evidence from large scale trials correlates closely with the evidence we see in our own clinic of children making dramatic gains (like the boy I mentioned here). And it does so without a lot of side effects (this is a topic for another blog, but our children have fun in our EIBI clinic… anyone who wants to know more about this is very welcome to buy a ticket to Grand Rapids, MI and see for themselves). Let me also be clear that ABA is not a wonder drug. Even very famous people tried it for the wrong things with disastrous results. Dr. Ivar Lovaas, the man who proved our kids could make double digit IQ gains and go from a 2% chance of mainstreaming to a 50% chance via 40 hours a week of intensive behavioral therapy, also tried to use ABA to “cure” children of unacceptable gender identities, with now unsurprisingly disastrous results. Moreover, if something does come along that out-performs ABA, you can bet that I will know about it before almost anyone, and that I will actively be planning to implement it in my programs and deliver it to the children who’s autism care I manage. Because my job is to help them thrive absolutely the best that they can.
In the meantime, my question is, why is anyone doing anything different? Why are there diagnosticians who work with children with autism who think that “good” practice is to prescribe them Risperdal, note every three months that they’re doing “well” (while they can’t hold a conversation and aren’t learning anything in school)? Why are there clinicians who put children with autism in other therapies (whether Floortime or Auditory Integration Training) as first-line therapeutic options because they “like” them? What on earth would make a clinician think that what they “like” or “don’t like” trumps the evidentiary basis?
I’m not a proselyte of ABA. It fits into a larger package for me. For young children with autism, who have limited skill acquisition and significant behavioral barriers to learning, it does better than anything, as monotherapy. If the children are aggressive, medications can help. If they are school age and learning, medications sometimes also help, particularly if they are dysexecutive in neuropsychological testing. If they are above a five year old’s verbal level, I’m thinking about getting them into team sports, martial arts, theatre or dance, and I’m thinking about giving their parents tools to help them make and keep friends. I’m thinking about getting them in our Puzzle Partners informal social supports programs, once their teenagers. I’m thinking about getting them through college and into professions.
But given the current state of the art, I think it’s completely absurd to be doing this without ABA, and until something better comes along, I shan’t dream of it.
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
This is a quick thought of the day, with apologies for good, solid blog posts being lacking from me over the past few weeks. Then again, it’s too much for me to squeeze into a tweet, and my mother thinks my blog posts are too long, so perhaps this will appeal to her!
They advance a very interesting idea that social networks function to extend and strengthen the secret connections that keep the wealthy (and dominant racial/ethnic/cultural groups) enfranchised. They do it by enhancing the ability of “who you know” to overpower “what you know” in being the person picked for the desirable job that becomes a great career or a stepping stone. It makes a lot of sense, since social networks allow easy access across strata of society to people, as long as they have the right connections (for instance, I routinely tweet with people who have 1/10 or 1/100th as many followers as me, or 10x or 100x as many followers as me, and we have a two-way interchange, although primarily because we are connected by the Autism Family). Without the right connections, however, Facebook, Twitter, and the like, are just as closed a door as any that existed before social networking.
We already know that people with autism are unemployed and underemployed compared to other people at their cognitive levels. This spans across the Spectrum — cognitively impaired autistic people are much less likely to work than people with MR without autism. High functioning autistic people with college degrees or graduate degrees are also less likely to work than their “neurotypical” peers. I talk to parents all the time about the fact that much of this has to do with people with autism struggling to read the unwritten messages and follow the unwritten rules in job searches. They rock out in their classes and get high grades, but they don’t talk to their professor or their peers about their interests. They don’t engage their departments to parlay their interests and academic success into internships, volunteering opportunities, and entry level jobs. This is all about unwritten rules and networking. Are we overlooking one of the most powerful tools thus far in the 21st century, in the form of these social networking sites, and what they may be able to do for autistic people?
We know (look at my timeline on Twitter, or check out the #AutismFlashFollow or #autismbullying hashtags!) that we have people with autism thriving on social media, as well as some who engage in it but are not engaged back. Maybe we need to think more constructively about helping people with autism develop social links on social media that are likely to generate jobs (because they may not automatically engage in using social media this way). Maybe the broader autism family needs to help build those links between people with autism on social media and the decision makers and other people who hold the keys to these invisible doors. What do you think? And if you’re an autistic person, have you used social media to land a job? Would you?
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
After the two day intensive autism workshop, I continued to make many great connections and learn a lot that I will be taking back to Michigan. The next three days of AACRC were definitely just as invigorating as the first two!
A significant part of the second half of the conference had to do with continuing to reduce restraint and seclusion in residential care. Residential care, for those less familiar (and it keeps a low profile) is an intermediate level of intensity for kids – mostly teens – who no longer have the acute stabilization needs that justify a psychiatric hospitalization but also are not ready or able to return to the community. It represents an ongoing process to make life for these kids both more therapy/improvement focused and also do this in a way that limits the restrictions placed on them. In the “old” days, these kids ended up in “institutions,” which were typically locked facilities, that, honestly, focused on warehousing children rather than helping them thrive. There was some limited therapeutic component to these programs, but the goal was rarely community re-integration, and most people who fell into this “system” we’re slated to spend the rest of their lives in it. There was usually little, if any attempt, also, for children to be engaged in the community, doing all the things their peers were doing, while still being based out of the treatment facility.
The “State Psychopathic Hospital” operated by the
University of Michigan in the early 1900s
The residential treatment center was a big improvement over the institution because it was designed to continue stabilizing these kids (and adults as well), give them skills, and teach them to function in the community, with the goal of getting as many kids as possible back into community placements – back to their birth home, to extended family, or into a new adopting family. Those who could not achieve these goals could still at least step down to a “group home,” where they would have freedom of movement and some self-determination.
Nationally, there a large number of kids in residential care. Actually getting a firm estimate, although these are individual American citizens, is surprisingly challenging. Magellan estimated that the number of children receiving this kind of care peaked around 250,000 in 2000. This number has been going down slowly over time, both due to cost pressures and due to programs that more effectively serve these kids in the community, and some sources estimate the number has gone down 30-50% in the last 15 years. Interestingly, however, there is substantialvariation from state to state in this practice, with some rarely choosing this level of care and some doing so with surprising regularity. Some people argue strongly that the goal should be complete elimination of residential care, over time. Others suggest that this is really a “right-sizing” problem in residential youth care, with some capacity that is not needed (because it’s in the wrong place or offers the wrong service) and some capacity that is needed but not available.
Residential treatment homes typically are still secured in some fashion – either via staff supervision of children by itself or this in combination with physical locks. This varies to some extent with the children (for instance, many of the nonverbal teens with autism we serve are very low functioning, and there would be significant injuries of them being hit by cars or otherwise injured if they were not closely supervised outside of the buildings). Kids frequently have their own room, for privacy, are allowed to have their own things, and participate in a range of regular-kid activities (dancing, sports, games, crafts) on the “milieu.” They also receive individual and/or group psychotherapy, physical, occupational, and/or speech therapies, and schooling. Kids in these programs typically have a fairly dense schedule of activities, including many opportunities to pick among activities (with some incentives to try a broad range of things, just like any parent would demand for their son or daughter). The staff members who serve them (typically in a low ratio of one staff member for every 1-3 youths) act in many respect like interim parents, and most programs allow teens to have a mentor or other formal relationship with that one staff member with whom they really bond. Some staff in some programs have been through this process themselves earlier in their lives, and other programs have peer advocates, so that teens have connections with people who know what it is like to survive and thrive through the “system.” On the negative side, most facilities do use some kind of physical management system (that is, some kind of holding or restraining of children). The best of these systems involve active efforts to avoid physically managing, or “laying hands on” kids, such as using verbal de-escalation, or specific talking tools that help kids help themselves. They also set firm limits on when physical management can be used, generally restricting it to a situation in which there is an imminent danger of the child harming the self or someone else, which cannot be resolved in another way besides physical intervention (See the system we use, the Satori Alternative to Managing Aggression, as an example; this system helps us frequently reduce management by 50+% over prior placements from which our kids transition, which is good, although the evidence basis for physical intervention is surprisingly weak, taken as a whole.) Some programs also use seclusion, or placing a child by themselves in a de-stimulating environment, to “cool down.” Although sensory rooms and other rooms designed to help kids manage their level of stimulation are great, secluding them is something we generally view this as even worse than restraint, because seclusion can be psychologically damaging. It is also particularly open to abuse, much like the solitary confinement system in prisons. However, even in the absence of seclusion, physical management of any kind is still something that the best among us view definitionally as a failure of our system. There were some great talks about taking this approach and creating a system of care in which even very aggressive, challenging behavior can be managed safely without physical intervention. The biggest component of this is actually just a determination (led by us directors and powered by influential leaders at all levels) to push to zero physical management, since this really pushes us to invest more and more in our ability to de-escalate. One of the big points made was that this was really a situation in which success required “shooting for the moon” – that aiming for any less than complete elimination of physical management just isn’t enough. On the other hand, it is very important to not just eliminate restraint without thinking carefully about how kids are kept safe and thrive in a restraint-free environment — one scholar aptly described this danger as “regulatory scotoma.”
Another great topic was working towards a situation where decisions to admit or discharge a child from residential care are made more systematically and consistently based on the interests of the child or adolescent, and not on other reasons like financial utilization management (either in the sense of the state’s desire to minimize expenditure or the facility’s desire to keep a bed full). There are some great evidence based tools slowly gaining acceptance for this. One thing that was particularly interesting was a “hinge plot” we saw, which showed the length of time for the symptoms of the average teen in residential care to reduce to “catch up” to the average teen in outpatient, community case management. (CCM is a service provided as part of mental health care, sometimes, to help people coordinate various kinds of healthcare needs, for those of you who’ve never run across it. UNICEF actually makes an interesting argument that it has applicability to non-psychiatric medical care as well, particularly in high risk populations.) Anyway, this bogey is actually pretty far out — well past a year, suggesting we may not want to rush to prematurely discharge youth, because this could lead to poor functioning in the community and re-admission, which has been shown to be an issue, this time, already in non-psychiatric aspects of healthcare. I don’t have a copy of that to show (yet), but other studies validate this idea. This Noftle (2011) study, for instance, does show fairly long stabilization timescales, although it suggests that residential care may be most effective for rapid stabilization over the first couple of months of children with the most severe behavior disturbance (this dovetails with what I see informally).
Other studies, like this one, suggest that there is a “time heals all” component to this process, and that intensity of service cannot arbitrarily shorten length of stay – rather, when this happens, the danger of needing re-admission (these quick trips in, out of, and back into the hospital are frequently associated with both bad physical and mental health outcomes). Interestingly, other studies show the rate of improvement in residential care and outpatient services are actually comparable, although there is some debate over whether the severity of issues teens in residential care deal with are being considered (generally, improvements are faster in “mild” treatment cases, so if RTC can deliver comparable improvement for severe issues in complex teens as CCM does for milder issues in simpler teen situations, this may actually be pretty good!). There is a particularly excellent review that is freely available through PubMedCentral from Sigrid James – her work raises important questions about the bar that we set for making sure that this expensive and restrictive kind of care is applied only where and when it needs to be.
Where these two issues come together, along with other issues such as the need to empower parents (about which I’ve already blogged), and the need to continue pushing for treatment approaches that are evidenced based, where available, and the development of evidence based practices, where none exist, is that twenty-first century residential care must make a better and better case for why we need to separate people – kids and teens especially – from their community roots. In the best of cases, residential care is a core component of a larger strategy to empower parents, give kids skills, and create an environment in which kids can learn to thrive without fear of catastrophic consequences of their mistakes, using residential care as a the plane ticket to a future that involves ongoing safety, a sense of permanent attachment to peers and adults who have made a long-term investment in the youth, and development of a true sense of well being. This requires a much more continuous system of care, with opportunities for teens to step up and down flexibly as they need to, to higher or lower acuities of service. It also requires some constructive thought about programs-within-programs or other techniques to much more tightly provide each teen with the services they need and pare down care that doesn’t take care of them (since that is not care at all). This is a lot harder in behavioral healthcare than physical healthcare, I think (a physician can learn when and how to safely prescribe five new medications far more easily than a psychologist can learn five new evidence based behavioral therapies), but it can and must be done. When we do that, we should sleep well, knowing that, one teen at a time, we are changing the world.
I hope these thoughts are not too random – this is a little of what I’m bringing home to think about improving our residential adolescent program to the next level, and far, far beyond, even as I fight harder than ever for the autism system I know our kids need.
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
I am fortunate to spend this week learning about innovations in children’s residential services, including a two day workshop on how to serve children with autism who need residential placement. (which just ended!) This is a tough part of what we do. I’d love to live in a world where residential services were not needed (and things like our EIBI clinic will slowly reduce the number of children, at least with autism, who need it!). But the reality is that these challenging kids will not thrive if our “A game” is not dedicated to them, and yet they’re frequently an afterthought. I only half joke when I proposed an alternate mission statement to my boss, that we take the kids everyone else gave up on, and we change the rules so that they, too, may thrive.
This is part of yet another weird paradigm shift for me in my career. Later this month, I’m sitting for the fourth and final phase of board certification in clinical neuropsychology (the ABPP system mirrors fairly closely the ABMS system in medicine, both systems recognizing specialists after they have completed the entire licensure process, to become psychologists and physicians, respectively). ABPP represents the culmination of a process I started 11 years ago to leave engineering (two years “catching up” on psychology via evening classes and learning psychology research at Wayne State University, four years at the University of Florida, a year at the University of Chicago interning and two years at Mary Free Bed Rehabilitation Hospital as a fellow, prior to my nearly two years at Hope Network). It’s been a long but tremendously rewarding road (and I agree with Neha’s tweet!).
All this left me knowing neurological injuries, neurodevelopmental disorders, diagnosis, treatment planning, developing a research program, and collaborating with physicians in a hospital setting, like the back of my hand. I did not expect (almost a year ago) to also take on the responsibility of overseeing and leading children’s residential services alongside my outpatient autism program. I have a great team, including the residential program director, Niki, who is just awesome. But, I have had a lot to learn! And that includes a lot of things I wish I didn’t know about the bureaucracy that surrounds the residential world. However, I love to dive in feet first. So if I’m going to lead residential, I’m dedicating myself to leading it far into this 21st century. And, hopefully, still manage to pass my neuropsychology boards, which will have nothing to do with any of this!
And thus, I came to New Jersey. The American Association of Children’s Residential Centers is the nation’s premier organization in this area, and I want to learn from and with the best. I’m going to lectures not only autism but Trauma Informed Care, treatment and discharge planning, aftercare, integrating medical and behavioral care, and several other topics.
As I mentioned, it all started with a two day autism fest. Which is, as Neha said, awesome. All-you-can-eat DRO, RIRD, and FBA (and you heard the way kids with autism speak can be repetitive and self-stimulatory!). Stimming / fidgeting toys at my table waiting for me at the lectures, too! I saw some great things that I’m taking home as I think about where I want our residential care to go next.
I love that everyone here is very humanistic in their motivation to serve kids woth autism who need residential placement. Like us, they work hard to understand behavior based on the premise that, when the function of problem behavior is learned, new behaviors can be taught or the behavior can be treated, rather than the child being labeled as a “bad kid,” and us moving into punishing crimes. I respect our police, judges, and so on, but punishing crime cannot be what we do.
One of the most consistent themes was a highly structured day, with organized transitions between activities, and play that hides teaching instead of excessive downtime. I think we do this well, but it’s a continual effort to do it better. I saw some great examples of how to push the envelope on structuring the physical space to make it more conducive to activity participation (while still being ruggedized for kids who destroy property!).
Speaking of the physical space, one small but great idea I saw was to use one’s own body as the visual analog scale for frustration or anger (that is, a very calm level might be anger at one’s feet or ankles, a moderate level at their belly button, a high level a their shoulders). We’ve all heard someone say, “I’ve had it up to here with you!” Beyond all the great things that just systematically quantifying anger does, using the body as a scale is great because it is ever present. And I personally also love the idea of developing a confirmatory code language with our kids that fosters our mutual goals. They can say, “I’m at my waist,” and their meaning is perfectly clear to us, to their loved ones, and to and each other but opaque to people who don’t need to know. As if that were not enough, we have been working on using the Soles of the Feet mindfulness approach, researched specifically for teaching anger management to people with cognitive deficits. It seems to fit perfectly, and between the two techniques, we could really teach our kids to walk on water!
I am sympathetic to the IT guys who are concerned about data security and respect HIPAA, but I really think we’ve got to move farther and faster to use solutions like Skype and FaceTime to not only connect kids in residential care with their family (which happens routinely) but also to do much more parent training, irrespective of distance, and for the kids where true family psychotherapy is possible, that as well needs to happen whenever it is clinically indicated, with distance as no excuse.
I’ve heard about a couple of models of aftercare that I want to explore farther. We deal with children who come from very far away, and we’ve met before with some innovators in distance aftercare, but one of the simple ones I really like is a hotline system where kids who are discharged have a lifeline back to that one staff with whom they really formed a bond (our kids have this staff formally assigned as their “mentor”).
One thing that bothers me a little is that only a few programs I’ve heard from really incorporate intensive behavioral therapy for skill acquisition (using either the applied verbal behavior framework, which our EIBI clinic uses, or the discrete trial training approach, which Ivar Lovaas and others pioneered). I don’t have a problem with sensory time in a residential program (and we do all kinds of sensory things, as reinforcers, just for fun, and for calming, even if I am not a proponent of “sensory integration”), but I really think this is the core of what we do for outpatient kids with autism, and I think using the residential environment to allow for this for kids who are not safe to remain in the community, too far from an outpatient clinic for multiple weekly visits, or simply have too much catching up to do, needs to be a big part of the focus.
Somewhat aligned with this is that programs seem to vary widely on who they admit, when, and why. This is a known, broader problem, although with autism being a relatively more homogenous population than the entirety of all kids receiving residential care, I had hoped for more ideas on systematically driving this, both programmatically and in the advocacy arena. I think we all agree that multiple, simultaneous problems exist. There are kids who are kept in the community too long, to their detriment and to their family’s, who could have had better outcomes with an early residential, intensive treatment approach, that would give them a better long-term trajectory that keeps them in the community. For these kids, who come to us late, unfortunately the residential door frequently swings only one way. There are also kids who are placed residentially for whom not enough work is done to keep them at home. And, there are kids who are placed residentially, but critical thought is not applied to what therapies and services they need, and so residential care becomes an extremely expensive way of melt detaining them, rather than helping them transform their lives.
I learned a lot of interesting things during the second half of the conference, which focused more on program design and providing high quality services to all youth in residential care.
So far, I really like AACRC. I’m definitely thinking about getting more involved, and I would like to see if I can’t present at next year’s conference.
This is an historical post from an earlier blog, Adopted Son of the Autism Family, which I had before this current blog. It is re-posted without modification (other than this introductory sentence).
The concept of investing is one that is pretty readily accessible to us. If you save $100 towards retirement when you’re 30, and you invest, it will be worth far, far more than $100 you invest when you’re 60. We prize early intervention for children with autism not only because they make radical gains when we provide intensive behavioral therapy at a young age, but because, if we change the teaching so they may learn (to paraphrase Lovaas), we can get them to a place where they can learn in traditional ways. That’s huge – for many of these kids, thirteen years of special education will not only be costly, but it will not produce great outcomes (this is not a dig against special education – it is a vital component of education, and a massive improvement over what has been done in the past – but any special educator would prefer their kids in mainstream classes if they could learn and function effectively there). In contrast, with EIBI, they can access 13 years of mainstream education, which will prepare them for college, professions, hobbies, and all kinds of other pursuits. So, that early investment has a big payoff.
Empowering parents pays dividends, too. Think about this. Parents who have a child with autism who have additional children have a one in four chance of subsequent sons having autism, and one in eleven for subsequent daughters. Just in my practice I’ve met many families with two kids on the spectrum, and even some with triplets, all with ASD. So in that latter case, obviously, tools like Pivotal Response Training or ImPACT (the video below is a GrandRounds presentation that Dr. Brooke Ingersoll of Michigan State University, who developed ImPACT, did for us) pay dividends, because if we can do parent training for a parent with three young children that addresses autism-related issues, training the parent once has a threefold effect.
But it doesn’t stop there. PRT and ImPACT are great tools, that produce evidence based gains for kids and families, but they clearly do not take the place of EIBI or other intensive behavior analytic therapies for most kids with autism. That’s why, while we provide parent training interventions, they are primarily used as a stopgap to getting children into EIBI. Once kids are in EIBI, parent training doesn’t end. Every time we are able to produce a skill and show sufficient generalization so that it occurs for multiple tutors on multiple days, we want parents to know what those skills are and when/how they can be elicited. We love it when parents take these lists home and memorize them – “if my daughter can do that for you, then she’s going to do it for me, and her mother, and her teacher!” If parents are struggling to elicit the same skills we can get in the clinic, we provide additional training, using one-way mirrors, our bug-in-the-ear system, and anything else necessary to transfer the ability to demonstrate the skill to mom and dad. When we do get kids listening, talking, engaging in gestural communication, socializing, and playing, via EIBI, we start immediately thinking about things like getting those children into structured physical activity, like team sports, martial arts, yoga, or theatre. We’re also thinking, right away, about helping them make and keep friends. How do we do that? We empower parents.
When I do psychotherapy, I often tell patients that I meet with them for an hour a week, and this leaves 167 hours a week when I’m not meeting with them. If I can’t teach them something they can use in those other 167 hours, therapy will not be that impactful. Even with the 10-40 hours per week of intensive therapies, there are still many waking hours outside of therapy. So, the first way that empowering parents is that it massively extends the range of therapy efficacy.
There is a second way that empowering parents pays dividends. As a clinician, I do a lot of battle with and advocating in front of insurance companies, community mental health agencies, the state, and to some extent, the federal government and nationally influential bodies, to try to fight for access to care. I have a little impact – people respect my title and my education, and the number of children with autism I serve (although I’m very early in my career, and others are far more experienced than I am!). But my voice is not impactful in those spheres like parent voices are. They will listen to me politely, and then ignore me. They may be rude to you, but they know they ignore you at their peril. Your voice matters. So, the second way that empowering parents pays dividends is that the blend of your passion and voice with our knowledge and skills is the ultimate advocacy weapon to demand the things we need to help people with autism thrive.
The mission I set for my Center is: The Center for Autism, through formal clinical services, informal support programming, research, and community advocacy, empowers families and transforms the community so that people with autism may thrive. These are just two ways that empowering parents is central to our mission. Clinicians, how are you empowering parents? Parents, how can we lift you up?