Here is a video of the Intersectional Feminisms and Masculinisms discussion, in which I had the privilege of participating recently, hosted by APA Divisions 35 and 51. I was glad to see some Division 44 friends in the audience, and glad to participate as a sister in the Division 35 tribe as well as in my role with Division 44. And, yeah, I said “ummm” a lot more than was necessary. Sigh. The other panel members are awesome though, you should go check them out.
Intersectional Feminisms and Masculinisms
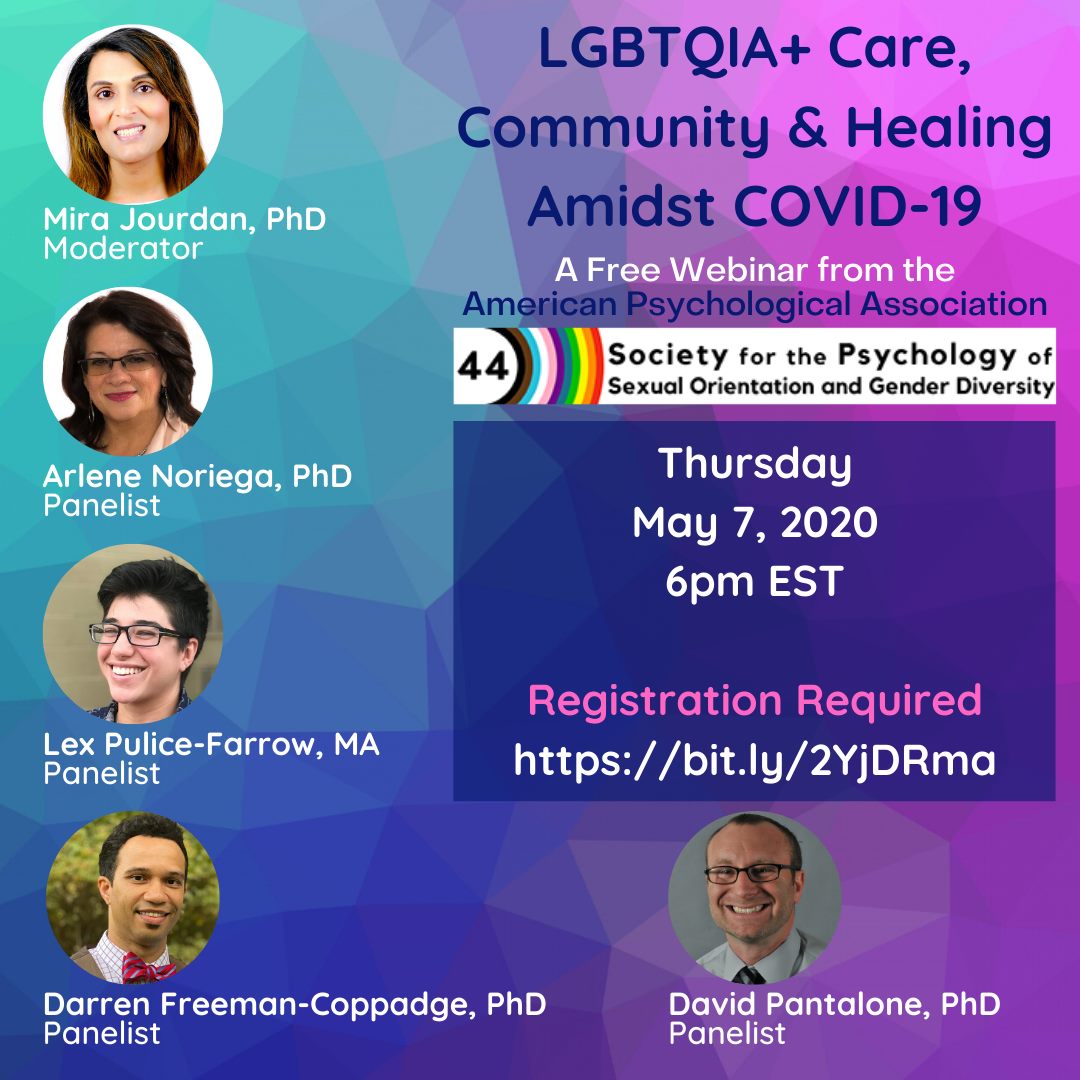
I’m excited to be a part of this upcoming online discussion in February. You can register here (sorry, the links in the image do not work).

Signatures to Show LGBTQIA+ Rights Matter
The day before yesterday, I had the chance to help host a very special Fair and Equal Michigan web event, featuring some amazing luminaries. We had current and former elected individuals, including former Governor Jennifer Granholm, former Presidential Candidate Beto O’Rourke, Oakland Executive David Coulter, and Jackson Mayor Derek Dobies, as well as my co-chairs, Jen’yce and Trevor, all shared personal and powerful stories in support of equality.
I used to be an avid cyclist (something I need to get back to!) and I was particularly thrilled that world-class trans athlete, Chris Mosier, was part of this too! So thrilled that I posted a quick fangirl snapshot to Facebook.

We interrupt this COVID-19 dining table workspace to fight for equality
We had amazing participants too, including multiple individuals who are running for office, themselves, as members of the LGBTQIA+ community or as allies. As I said on the call, I just cannot believe I get to be part of events with other powerful advocates like these.
You can still sign Fair and Equal Michigan’s ballot initiative. It takes only a minute, and you can do it online.
Mira Krishnan LLC does not engage in partisan activities, and this post is not intended to endorse any party or candidate for office.

With love, sorrow, remembrance, and commitment
Self-Healing, Growth, and Advocacy in the Pandemic: Psychologists Share
Yesterday, we hosted a wonderful webinar with The Society for the Psychology of Sexual Orientation and Gender Diversity (APA Division 44), where a panel of psychologists and trainees across career phases discussed their experiences during the COVID-19 crisis. Our focus is on the experiences of gender and sexually diverse psychologists, as well as on service to LGBTQIA+ patients, but I hope this is useful to practitioners and servants from many different backgrounds. I had the privilege to moderate a panel of my distinguished colleagues. They shared how they are caring for themselves – from taking joy in their families to reinvigorating their mindfulness practices. They shared growth in their understanding of themselves and their role within their communities. Frustrations, they had too, and they shared limits in being able to care for patients, from barriers to providing telemedicine to rural and poverty-affected patients caught up in struggling with the unintended consequences of social distancing and shelter-in-place orders. We discussed feelings of being sidelined as behavioral health providers and teachers, in this crisis, recognizing advocacy opportunities this situation brings, and, together with our attendees and fellow Division members, we talked about how we can do more. Check it out!
Oh! Two more things. Besides making sure the community has access to and can process empirical science, and helping individuals and communities manage the major life changes and behavioral interventions COVID-19 has required, psychologists have been working together with our many siblings-in-arms to recognize, address, and minimize disparities in access to care and in who gets an opportunity to thrive during this challenging time. The hashtag is #EquityFlattensTheCurve, and you can follow this link to find out more.
And, finally, to everyone out there: whether you are on the front-lines of face-to-face crisis healthcare delivery, whether you have been able to implement telemedicine to continue to support others, whether you are doing some other kind of essential work, from home or from your regular place of work, or whether you are just helping your community by practicing social distancing and sheltering at home, or by everyday acts of love and kindness for your family and neighbors. You are loved. You are valued. No one may ever truly understand the sacrifices you are making, but you are heroes to us.
Love and Telemedicine in the Time of COVID
I have served for a number of years on the board of the Association of Children’s Residential Centers. Our raison d’être is serving complicated youth and their families, and doing it with heart. These organizations provide typically very “high touch” services to youth going through crises. COVID-19 has been particularly challenging in some unique ways – most of these organizations continue to serve youth, but there are many considerations for doing so safely while making sure we are fully supporting youth and their families during a very critical time in their lives. Late last month, alongside colleagues from other member agencies shared our experiences using telemedicine.
Although I was not doing telemedical services right at the time I moderated this, I have been conducting some select services via telemedicine since then. It is a truly complicated undertaking on many levels, ranging from HIPAA compliance to communicating expectations clearly to patients. On the other hand, many organizations, including the American Psychological Association, have stepped forward to help practitioners figure this out.
For me, personally, I have found this very rewarding, and my patients have been very open and collaborative in dealing with these uncertainties with me. It makes me feel more connected to the people I serve. They are in need, and this is a safe, if imperfect way to do it. Selfishly, and something that I want to spotlight on a different webinar (with a different partner) later this week, it also helps me deal with my own sense of uselessness during this crisis. Much of my engagement has been online – at first, getting people to take this crisis seriously, helping guide people to accurate and scientifically informed data and helping them understand the limitations in what we know. I’ve continued advocating for the disability communities whom I serve online. However, I’m used to being on the front lines – I spent almost the entirety of my training (seven years) in hospitals (and before that, on a different front line, in the manufacturing world), and it’s only been the nine years since then that I have not been on the front lines.
Here are our thoughts, and our encouragement. It is still a good time to think about these issues and consider launching telemedicine services.
Edit: I quickly created this post last night, while ensuring panelist permission to publish this, and in the morning, I also saw this great piece from Dr. Rosenthal, a pediatrician at Yale. I don’t usually see infants, but I see many toddlers in my practice, and like her, I find so much rewarding about being connected to my families via telemedicine, and also frustration – it will be a long time before camera technology is adequate to give the kind of in-the room “Witcher sense” we all have, and allow us to notice all the subtle things about our patient’s breathing, subtle changes in their attention and affect, and all the other cues that are so important to doctors like her and myself.
Edit 2: The next day, Washington Post ran this excellent piece for patients, helping them understand what care might be put off, what care should not be put off, and what care is and is not appropriate for telemedicine. That last point is a critical one, which we touched on briefly in the webinar, too.
As I noted in other recent blog posts, Mira Krishnan LLC has been using various partnerships to assist with as well as produce webinar content that helps advocate for embracing, supporting, and empowering special populations, all within our longstanding goal of powering up the world through diversity. If you want to work with us, let me know!
Upcoming Webinar! Supporting Providers Serving Gender and Sexually Diverse Patients
As I mentioned in my last blog post, I am working on a number of webinars to support diversity during the age of the quarantine. I serve as President Elect for the Society for the Psychology of Sexual Orientation and Gender Diversity (AKA Division 44 of the American Psychological Association), and I am moderating a wonderful panel supporting providers serving gender and sexually diverse patients (the LGBTQIA+ community) later this week. Registration is still available, and because we are so passionate about getting this in front of providers, and with tech support provided by Mira Krishnan LLC, we are making this available free of charge. You can register here.
Oh yeah, you guys, I am playing with a new simplified logo. What do you think?
As I mentioned in my last blog post, if you would like to partner with Mira Krishnan LLC on a webinar, reach out to me. Our emphasis is on enhancing diversity via changing public attitudes, providing professional education, and increasing opportunities for minority populations.
Supporting Diversity via Immigration Education
One of the things I have been trying to do, via Mira Krishnan LLC*, is to use webinars as a format to continue my mission of diversity education during the COVID-19 crisis. I helped the Association of Children’s Residential Centers plan a recent webinar and moderated panelists discussing implementing telemedical services for youth with complex challenges and their families. I will be hosting a webinar for the Society for the Psychology of Sexual Orientation and Gender Diversity (of which I am President Elect) supporting the community of providers and psychology trainees supporting LGBTQIA+ patients. Webinars hosted by Mira Krishnan LLC are non-partisan and educational, and generally focus on some element of supporting diversity and diverse populations.
This weekend, I had the wonderful opportunity to host a webinar with GC Reforms, a non-profit organization dedicated to reforms for the United States immigration system.
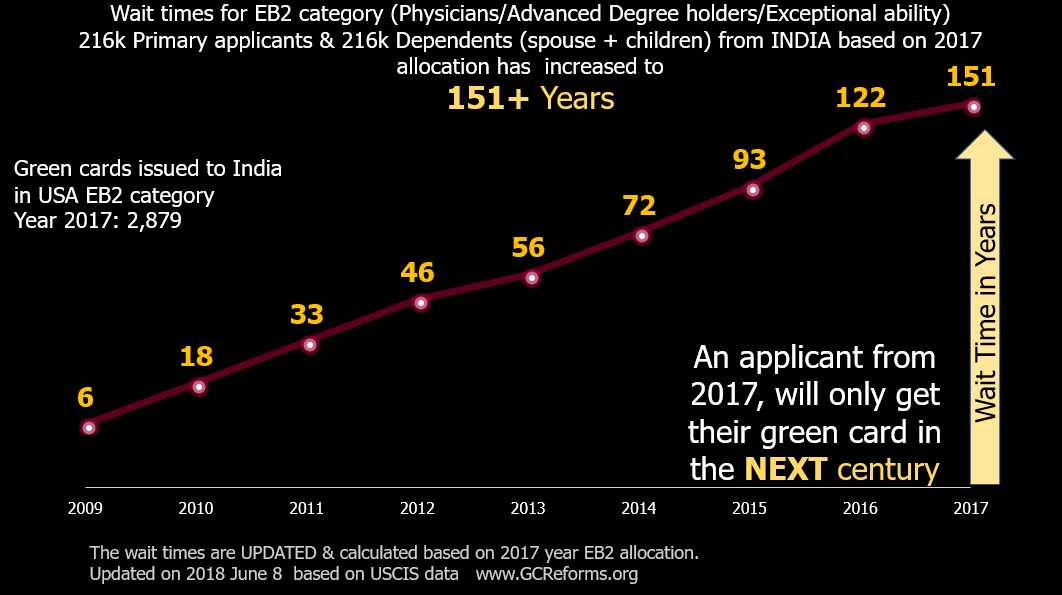
This graph, from GC Reforms, shows that wait times for Indian-American immigrants have become so long that they are much longer than the human lifespan. This means the average skilled worker trying to obtain citizenship from India will die before becoming a US citizen.
Because of the way the system works, and because it has not been overhauled in nearly 100 years, the system is heavily biased against high-skill workers, particularly when they come from large countries, such as India and China. These are knowledge workers from a range of industries who have tremendous gifts to give to US employers. They are here, already, on work visas. They pay US taxes. They have followed every step of the immigration process carefully. And yet, because of the way this system works, they can expect to die before they will be granted US citizenship. This is unfair to them and to our country. To find out more, watch the video, below.
If you have suggestions for additional content you’d like to see in webinars, please reach out to me! This is just one small way I am trying to support diversity, even in the age of quarantine.
* You guys, I recently became a Mira Charlotte Jourdan, but the LLC is keeping its name for now. To quote the Elvis Costello song, you can call me anything you like, but my name is Mira.
All I Learned at Camp Grad School
A few days before the world dramatically shut down in response to COVID-19, I had the opportunity to take the stage at LaughFest, and share a short story, as a part of their “(No) Laughing Matter” series. Here it is.

Mira’s first and last attempt on a comedy stage? Or is it invariably comedy when I speak?
I’m a neuropsychologist – a kind of psychologist who specializes in applying neuroscience and understanding brain development and injury. I want to tell you a little bit about my life when I was in grad school. Neuroscientists like to say the human brain is the only organ that can study itself. So you should know two things about my brain in those days.
The first is that I hated kids. I couldn’t stand them, and I suspected the feeling was mutual. I may not have mentioned that a big part of the work I do now is with preschoolers. The second thing is that I had been suffering from an eating disorder for about five years prior to grad school, and I was early in my own recovery.
None of this is rational. There’s no rational reason to like or not like kids. Well, I guess if we all didn’t like them, that would be bad. I mean, we were all kids once, and thank God somebody liked us. Most of us. But not everyone needs to like kids. And there’s a perfectly rational and sensible reason to eat when you’re hungry – most anything else is irrational. But as I lost more and more weight, I was pretty good at this irrational thing. I did crazy things, like working all day in Troy, taking night psychology classes, and then driving down to Wilmington, OH to try and save a failed engineering project (which I did). And, well, packing a scale in my suitcase so I could weigh myself after dinner and decide if I needed to throw up. And counting calories. Obsessively. A four-hour drive is a long time to count calories, and when I did stop, I knew everything low-calorie there was in all of those convenience stores, but I could still stare at the nutrition labels for ten minutes or a half hour to figure out what I was willing to eat. That ten-calorie difference between two energy drinks means the world. All of this was crazy.
That’s the thing. I knew perfectly well how irrational my behavior was. And I knew I was making bad decisions about my own body and my own mental health, even as I was learning to help other people make good decisions. I didn’t stop being crazy smart when I was crazy, and I had the grades, test scores, even a publication or two to prove it.
You can watch yourself – acting crazy – it doesn’t make it any less crazy, even though the part of you that is totally sensible is seeing all of this happen. There’s even science to prove this. As one example, a scientist gave people with anorexia and healthy people this test where they had to judge door sizes and who would fit through what door. They were both accurate when judging other people. The anorectics only made mistakes when judging themselves. And there are always external referents. When you get so thin that you can’t find any clothes that fit, and the small sizes are like tents on you, that should probably be an indication of something, right? But not for me.
But there I was, working crazy hard in grad school, trying to be a little better, by which I meant I would stay up all night doing research work in the lab and try to get by on an ice cream bar in 12 hours, but I did eat. I made an attempt to get healthier as I got closer to doing clinical work, but then there was this other thing. I’d be starting my clinical work seeing kids, whom I hated. My experience of children basically amounted to my church telling me I was in charge of the nursery, and then whoever sent me down there throwing me in the room, closing the door with all the crying children, and laughing as they ran down the hall.
So, like anyone who stays up all night in the lab on an ice cream bar and who will turn anything into a project would do, I dove in. I looked for what I could do to get by at working with kids and started volunteering at a camp for kids with serious illnesses, where I probably spent several thousand hours over the course of my grad school.
That first summer, I stayed a week at asthma camp. It was an easy pick – the little kid who lived next door when I was a kid had asthma. I learned English because I wanted to talk to him through the fence, when we were two years old. And here I was, the kid hater with a cabin full of extremely hyperactive little kids with asthma.
I got assigned to two little boys who were obsessed with swimming. All day, into the pool, out of the pool just long enough to get to damp swimsuit time, and then back in. Florida is not great for curly hair, and pool water does not help. Oh, yeah, and also I can’t swim. I was really scared of deep water as a child, and I always found some way to worm my way out of having anything to do with it in swim class in school. But these two boys wanted deep water swimming bracelets. So when they were ready, I had to go with them.
The day they were ready came pretty quickly, and it was all of a sudden, and I didn’t have much time to think. All I thought was that there was a lifeguard on duty, and what was the worse thing that could happen? So in they jumped, and in I jumped after them. And swam. Through the deep water. And they got their bracelets (I would like to point out that no one gave me a bracelet!). And we had a ball. And ever since that day, I’ve loved deep water – I pretty much picked up treading water in the deep end of the pool with them, that week, and after that, every chance I could get, I would swim at camp or at the pool in our complex. I would even swim in the rain – you’re already wet. Except I didn’t understand that it doesn’t rain without lightning in Florida, so I got a lot of “Hey, you! Get out of the pool! Are you crazy?”
It worked, too. The first thing is that when I learned how to play with those kids, it turned out, most of the time, I was pretty good at it. I ended up in charge of the woodshop a lot. I am a terrible carpenter. There are all these dads in there, who basically make projects for kids. But I can’t, and so all I have left is to make it a fun experience, together. If you ever get me to help you, you will go home with the most God-awful monstrosity your parents have ever thrown out on the way off camp. And the best memories.. By the time we started clinic that fall, the upper year grad students thought I was a child psychologist. And, well….
Those kids, and my patients in general, became a huge motivation to be healthy that things like not being able to find clothes that fit, endless, bottomless hunger, and weird moments where you’re outside of your body watching yourself eat peanut butter (the worst of all losses of self-control), just plain were not. I became progressively healthier over the course of grad school. I didn’t formally do therapy until my internship year in Chicago, but by then I was serious about wellness.
Those days changed my life in interesting ways. I did not foresee myself doing work where two-year olds crawl onto my lap and then fart – grad school did not prepare me for how bad preschoolers can have gas. And I didn’t expect to learn to love my body without needing to attach a number in pounds or kilograms to it. Rational me wouldn’t be here. The magic of neuroscience is that my brain got to experience this and live through it, at the same time.

Here is the whole crew of talented artists, surrounding Teresa Thome and Tommy Allen, who curated the event. Thank you, guys!
My appetite is stable these days. When I gain weight – which was a problem for me last year, I have to work double hard to ignore all the dieting memes. That part of me is still in there, and you give her the opportunity to take charge, and I will be right back where I was fifteen years ago. That skinny bitch on the inside is tough, and I don’t trust her, even as I miss being her. But I almost never listen to her, and I’ve stayed healthy.
If there is a lesson, it is to embrace the fact that you are irrational, but try to know what you’re irrational about. Be crazy at the right times. And if life hands you two kids who want to spend all their time in the swimming pool, jump in the deep end. You may not even need the lifeguard, and it’s sure to make for a good story.
Stroke and Return to Work

Although return to work seems to frequently occur in spite of some level of cognitive issues and emotional distress, more significant issues need to be considered to identify those who may have the most difficulty succeeding (image: Fotolia)
Data suggests strokes, or cerebrovascular accidents, are becoming more common in younger adults. Many people successfully return to work after a first stroke, and data suggests that many do so in spite of some level of mild issues with cognition, as well as mild anxiety and/or depression, but more significant issues in these areas can be predictors for who does and does not succeed in returning to work. Understanding the specific task demands, including cognitive and social / interpersonal skills needed, for a specific premorbid employment can be an important key. Read more in a new blog post on my forensic practice site.
